LOVE YOUR HAMSTRINGS: Hamstring Strain, ACL Injury, and PFPS
This is for anybody that likes a good story. This discussion will be educational and informative for those who do not already have a background in human anatomy, but will also provide interesting new viewpoints to a seasoned physical therapist, personal trainer, or any healthcare professional. This piece will begin as a story but will progressively get more technical and based in biomechanics. I have included several common analogies and implemented a story-telling style to, again, ensure inclusive understanding by any audience. I also ask for research and biomechanics from the audience (especially where I insert “COMMENT BELOW”). I am happy that I finally decided to put these thoughts into words and compile this 20-25 minute read, as it provides a great opportunity to shed light upon the many different mechanisms of injury, supportive research, and biomechanical analysis that surrounds the knee joint. This piece was inspired by my experiences with patients, clients, athletes, and everyday people--for whatever reason, it’s difficult for most to appropriately use those 4 long muscles that stride the femur.
Four muscles with many jobs attached at the back of your thigh? It’s the hamstrings. The importance of this muscle group is immense--from ACL injury prevention to optimizing performance--these muscles need to be used properly! You’ve probably heard clients or strangers complain, “my hamstrings are sooo tight!!!” and they proceed to stretch them periodically. This may make them feel relief temporarily, but once they realize that this level of stretching is unsustainable and feels more like pulling teeth, they truly see that basic stretching may not be doing much at all.
At the end of this journey, we will tackle the best ways to “make these muscles awesomer” (and no, it’s not by forcing yourself to touch your toes in the shower). But before we begin, we will need to review some basic anatomy, explore evidence based reasoning on why it’s even crucial to improve these muscles, and learn about the involved biomechanics.
Hamstring Anatomy:
These 4 images of the 4 hamstring muscles below are from breannaspainblog.com--they’re awesome. These images depict the textbook muscle attachments, but as I’ve discussed in “EPISODE 4 BIOMECHBBALL - DOWN THE RABBIT HOLE”, there can be variability in our soft tissue structures (muscles, tendons, ligaments, other connective tissue) from one human to the next. In general, though, the hamstring muscle group lies on the posterior (back) aspect of your femur (thigh bone), and each muscle in the group does something a little different depending on where their tendons specifically attach. It is best to think of muscles as lever systems, each with at least two attachments. The muscle belly is connected to a bone by tendons. Together, the tendons pull the attachments of the muscle and bone closer together. The rule is, if a tendon crosses a joint (where two bones meet) it will move that joint. For a hamstring to be considered a hamstring, it has to attach to a specific bony prominence on your pelvis called the ischial tuberosity. You may remember a time when you plopped down too fast on a hard surface and you felt like you have bruised a bone--those are your ischial tuberosities. This allows all 4 hamstring muscles to move your hip, as they all attach to the ischial tuberosity and their associated tendons have to cross over the hip joint to get there.
I think we are ready, let’s dive in…
 THIS IS MY FAVORITE MUSCLE IN THE ENTIRE BODY. The almighty adductor magnus. The implications of this muscle’s attachments are huge. Let me walk you through...if you look at the top left portion of the picture where it says “proximal attachment” and go down to the “hamstring part” of the muscle, you will see the word ischial tuberosity. The difference between proximal and distal attachment can be confusing if you don’t know the anatomical position of the body, but for our purposes, the proximal attachment is closer to your belly button, and the distal attachment is further away from your belly button. If we look in the top right corner under “distal attachment” and move down to the “hamstring part”, you’ll find two bony landmarks that are above your knee. THE ADDUCTOR MAGNUS IS THE ONLY HAMSTRING MUSCLE THAT DOES NOT CROSS YOUR KNEE. Therefore, it is the only hamstring muscle that will neither move your knee nor be affected by knee movements. In the bottom right, you will see the muscles actions, and they are hip adduction (like crossing one straight leg over the other straight leg) and hip extension (like you are swinging your leg back before you kick a field goal). The adductor magnus, along with the gluteus maximus, actually have the largest cross sectional area (muscle size) out of all of the primary hip extensor muscles. The ability for the adductor magnus to extend the hip increases as the hip is flexed (when your leg is swung forward after you’ve kicked the ball) to 60º.22 To summarize: the hamstring portion of the adductor magnus has tendons that attach from the ischial tuberosity to above the knee joint on the inside of your leg, crossing and moving only your hip joint.
THIS IS MY FAVORITE MUSCLE IN THE ENTIRE BODY. The almighty adductor magnus. The implications of this muscle’s attachments are huge. Let me walk you through...if you look at the top left portion of the picture where it says “proximal attachment” and go down to the “hamstring part” of the muscle, you will see the word ischial tuberosity. The difference between proximal and distal attachment can be confusing if you don’t know the anatomical position of the body, but for our purposes, the proximal attachment is closer to your belly button, and the distal attachment is further away from your belly button. If we look in the top right corner under “distal attachment” and move down to the “hamstring part”, you’ll find two bony landmarks that are above your knee. THE ADDUCTOR MAGNUS IS THE ONLY HAMSTRING MUSCLE THAT DOES NOT CROSS YOUR KNEE. Therefore, it is the only hamstring muscle that will neither move your knee nor be affected by knee movements. In the bottom right, you will see the muscles actions, and they are hip adduction (like crossing one straight leg over the other straight leg) and hip extension (like you are swinging your leg back before you kick a field goal). The adductor magnus, along with the gluteus maximus, actually have the largest cross sectional area (muscle size) out of all of the primary hip extensor muscles. The ability for the adductor magnus to extend the hip increases as the hip is flexed (when your leg is swung forward after you’ve kicked the ball) to 60º.22 To summarize: the hamstring portion of the adductor magnus has tendons that attach from the ischial tuberosity to above the knee joint on the inside of your leg, crossing and moving only your hip joint.  The biceps femoris...yes you have biceps in your legs. Let’s break down the word bicep. The prefix bi- means two and the suffix -ceps means heads. So, one muscle with two muscle heads, a short head and a long head. Why are the short and long head not considered to be two separate muscles? This is because both heads have a common distal tendon that attaches to 3 lateral structures. These distal attachments cross over the knee joint, so both heads of the biceps femoris will move the knee joint (remember the rule). However, each head has different proximal attachments, leading to the distinction between short and long heads. The short head of the biceps femoris (named for its short tendon) attaches to structures below the hip joint (not the ischial tuberosity), while the long head of the biceps femoris (named for its long tendon) does attach to the ischial tuberosity. Thus, it can be concluded that ONLY the long head of the biceps femoris is a hamstring muscle, since our rule states that you are hamstring muscle IF AND ONLY IF you attach to the ischial tuberosity. Therefore, for the purposes of this story, when we discuss the biceps femoris as a hamstring, we are primarily concerned with the long head. This muscle will extend the hip, flex the knee (bring your heel to your butt) and laterally rotate the hip and knee (facing the inside of your leg forward).
The biceps femoris...yes you have biceps in your legs. Let’s break down the word bicep. The prefix bi- means two and the suffix -ceps means heads. So, one muscle with two muscle heads, a short head and a long head. Why are the short and long head not considered to be two separate muscles? This is because both heads have a common distal tendon that attaches to 3 lateral structures. These distal attachments cross over the knee joint, so both heads of the biceps femoris will move the knee joint (remember the rule). However, each head has different proximal attachments, leading to the distinction between short and long heads. The short head of the biceps femoris (named for its short tendon) attaches to structures below the hip joint (not the ischial tuberosity), while the long head of the biceps femoris (named for its long tendon) does attach to the ischial tuberosity. Thus, it can be concluded that ONLY the long head of the biceps femoris is a hamstring muscle, since our rule states that you are hamstring muscle IF AND ONLY IF you attach to the ischial tuberosity. Therefore, for the purposes of this story, when we discuss the biceps femoris as a hamstring, we are primarily concerned with the long head. This muscle will extend the hip, flex the knee (bring your heel to your butt) and laterally rotate the hip and knee (facing the inside of your leg forward). 
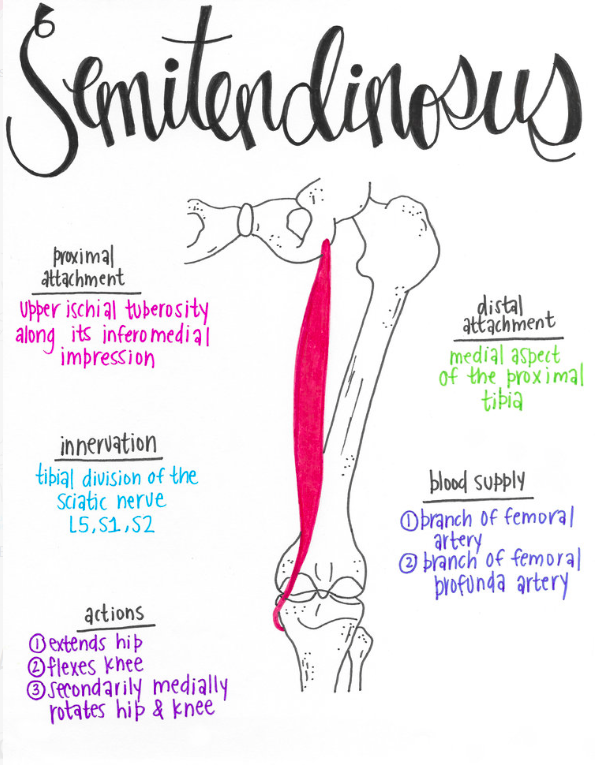
Moving onto the semis… semimembranosus and semitendinosus, that is. These two muscles, as you can see by their arrangements, are very similar. How they differ is in their specific distal attachments. The semitendinosus attaches distally to the medial aspect of the proximal tibia. This bony landmark is also called the pes anserine. Fun fact--pes anserine means goose foot in Latin, named so for its 3 muscle attachments. It also has its own bursa (a fluid-filled sac to prevent friction). The two other muscles that attach to the pes anserine are the gracilis and sartorius. The pes anserine can be a tender source of pain. The semitendinosus and semimembranosus differ from the long head of the biceps femoris in that they act to medially rotate the hip and knee (facing the outside of your leg forward).
The long head of the biceps femoris, semitendinosus, and semimembranosus are called two-joint muscles. As we reviewed, these muscles will in turn act on both the hip and the knee. Another important implication of two-joint muscles is that they can be shortened and lengthened differently at each joint. For example, when you squat, you are simultaneously flexing your knee and hip on the way down. Therefore, you are simultaneously shortening the long head of the biceps femoris, semitendinosus, and semimembranosus distally at the knee, and lengthening them at the hip. So, in theory, if you are flexing the knee and hip the same amount, the lengthening of one side of the muscle and shortening of the other side of the muscle will cancel out and produce a net change of zero in total length, which in turn will not affect the depth of your squat.
If we go back to the adductor magnus however, this is a one-joint muscle. Thus, this muscle, theoretically, CAN limit your squat depth because as you flex your hip on the way down, you will stretch this muscle. To get some context, stand up and do a classic hamstring stretch. Reach down and touch those toes with your knees straight (or as best as you can). Now bend your knees and feel the tightness go away--you are now putting the three, two-joint hamstring muscles on slack. That’s good enough for now...let’s get into why we need to “make these muscles awesomer.”
Injury Prevention/Performance Optimization:
Injury prevention is optimizing performance. As you read this section you will see how these two ideas go hand in hand. The key to both of them is to improve muscle strength in multiple ranges of motion. Is this even important? Do we truly need improved muscle strength to prevent injuries? It has been recognized that preventative based intervention programs can decrease injury prevalence in many athletic populations. Since this is biomechbball, let’s look at a study done on basketball players. A 2015 systematic review (a study that attempts to collect previously done research in order to connect information regarding a subject), aimed to collect and analyze the most recent research on prophylactic (preventative) intervention programs and their effects on diminishing injuries in basketball players. This study concluded that these interventions did indeed decrease the prevalence of various lower extremity based injuries and ankle injuries amongst basketball players.28 The interventions described in the study were mainly muscle strengthening programs. So, it is doable, but why does it work? This depends on what injury we are talking about. For example, in preventing hamstring strains, ACL injuries, and even patellofemoral pain syndrome (PFPS or chondromalacia patella), appropriate hamstring strength in many ranges of knee motion is necessary.
Let’s look at hamstring strains. First of all, what is a muscle strain? It is basically just
overstretching or tearing muscle fibers within a muscle. The idea is, if you try and contract a muscle forcefully, especially at a range where you do not have enough strength in that muscle, a muscle tear will be the result. A 2004 study aimed to predict hamstring strains in elite athletes with previous unilateral (one-sided) hamstring strains. They compared 9 athletes’ previously strained hamstring to their unstrained hamstring and to 18 uninjured athletes. The study examined the athletes’ mean optimal angle in order to produce peak torque in the hamstrings (the best knee angle in which each limb can produce the greatest rotational force). The only significant difference that this study found was that the optimal angle for peak torque capped at significantly shorter muscle lengths (greater knee flexion) in previously strained hamstrings than in non-previously strained hamstrings. Each of the individual 3 means measuring optimal torque angle for each type of uninjured limb (2 uninjured limbs in the uninjured athletes, 1 uninjured limb in the unilateral hamstring strain athletes) were 30.1, 27.3, and 29.8. Whereas the mean optimal angle for peak torque in the previously injured hamstring was 40.9.6 Additionally, a 1993 study assessing injuries in elite level Australian football players, found that a lack of hamstring strain history correlated with a 16% susceptibility to a future hamstring strain, whereas a history of a previous hamstring strain increased this probability to 34%. 26 To summarize, the 2004 study concluded that previous hamstring strains are correlated with peak knee flexion strength at greater degrees of knee bend then non-injured hamstrings, and the 1993 study concluded that if a previous hamstring strain has occurred, there’s a higher chance of developing an additional strain. Combining these two conclusions, it is more likely to get a hamstring strain if the muscle does not have adequate strength in greater ranges of knee motion. This makes sense.
 If you have never seen a hamstring strain in basketball before, here is how it happens...take a look at Chris Paul on the left, who has suffered many hamstring injuries throughout his NBA career. Imagine that left foot landing and slipping forward. This will cause his two-joint hamstring muscles to elongate. The same muscles will then contract as a protective mechanism of the knee joint; but, if they contract in this newly elongated position, and he does not have the available muscle strength in greater ranges of motion, his hamstrings will tear. This may especially occur while playing basketball as your hamstring strength may diminish as the game continues.14
If you have never seen a hamstring strain in basketball before, here is how it happens...take a look at Chris Paul on the left, who has suffered many hamstring injuries throughout his NBA career. Imagine that left foot landing and slipping forward. This will cause his two-joint hamstring muscles to elongate. The same muscles will then contract as a protective mechanism of the knee joint; but, if they contract in this newly elongated position, and he does not have the available muscle strength in greater ranges of motion, his hamstrings will tear. This may especially occur while playing basketball as your hamstring strength may diminish as the game continues.14
Connecting these two pieces of evidence may have important implications for strength and performance training. Looking further, we can find evidence that having improved hamstring strength increases performance. In Kean et al, they examined the effect that a simulated basketball game had on the effects of hamstring strength and its relation to athletic performance. The changes they found in hamstring and quadriceps strength were not statistically significant. The correlations that the study did find were the following: there were significant moderately positive relationships between changes in sprint performance and changes in dominant hamstring muscle strength, as well as dominant hamstrings:quadriceps (H:Q) ratio (the relative strength of the hamstrings to the quadriceps). Furthermore, significant moderately positive relationships were displayed in jump performance and changes in dominant hamstrings strength, non-dominant hamstrings strength, and non-dominant hamstrings:quadriceps ratio. Basically, the diminishment in hamstring strength relative to baseline and compared to the strength of the quadriceps, is associated with decreased athletic performance. To even further clarify--if you want to jump higher and sprint faster, you need to improve your hamstring strength, and involve our hamstrings within your motor plan.14
In my experience playing basketball, coaching, and working with clients, patients, and players, it is much easier to use your quadricep muscles than your hamstring muscles. For me personally, it takes a lot more effort to elicit lumbopelvic control in order for my hamstrings to be activated. Lumbopelvic control sounds pretty complicated, but this just means to execute on your intent to either move or stabilize your pelvis and lumbar spine. By moving your pelvis, you are moving the ischial tuberosity, which is shortening or lengthening your hamstring muscles. The moment before you want to forcefully contract a muscle, you naturally would want to put that muscle into a stretched position, but only for an instant. Stand up and try to jump as high as you can. You’ll notice that you bent down first before quickly jumping into the air. You were activating the stretch reflex. By stretching a muscle and then quickly contracting it, you will utilize the powerful advantages of the stretch reflex. There is probably a couple of things happening to contribute to this phenomenon. One is that this reflex is a neurological protective mechanism that is trying to inhibit the amount of range that joints are going through in order to prevent injury. Another reason is likely the viscoelastic nature of muscles, tendons, and connective tissue. This allows for a rubber band or spring-like effect.
Let’s relate this to some things that happen on the court (the piece of my beautiful art on the left of the screen). The starting position on the left of the drawing represents the “triple threat position” (the position before you do something with the ball). The black line represents your hamstrings and the triangle represents the pelvis. In the starting position you should have some posterior pelvic tilt with subsequent lumbar flexion (your hamstrings are shortened). To simplify, your spine is curved in the starting position. The ending position, on the right of the image, shows the lengthened position of the hamstrings from the pelvis to the pivot leg. You want to take advantage of the stretch reflex, so you innately want to start in the first position. If you were to start in the second position, it would be like trying to jump as high as you can but starting bent down--losing the opportunity to use the stretch reflex. You would be stuck to the ground like glue! For example, to take advantage of the stretch reflex and get past your defender in basketball, you would begin in the first position and then move into the second position only for a brief moment before exploding past your defender.
Earlier I was discussing the importance of hamstring strength for jump and sprint performance. I also mentioned the hamstring:quadriceps ratio (H:Q). This ratio may have some importance for performance and injury prevention, but first let’s define some terms. There are two types of ratios; conventional and functional. The conventional ratio shows the balance between the quad concentric (muscle shortening) strength and the hamstrings concentric strength. When optimal, the conventional ratio has been shown to be at least .6 H:Q (3:5). The functional ratio refers to the hamstring eccentric (muscle lengthening) strength as compared to the quad concentric strength. A functional ratio of 1.0 may indicate greater joint stability.1,2,8,9,24 To put these numbers into context with the hamstring strain, there was a study done on 462 professional soccer players. They measured their quad and hamstring’s concentric and eccentric strength. Of the players that had preseason H:Q imbalances, they’re injury rate was 16.5%, whereas the players without preseason H:Q ratio imbalances had an injury rate of 4.1%. Also, players who had a preseason H:Q functional ratio of 1.40 or higher did not get injured.9 This was a great study that correlated a vast amount of information, but you get the idea. We will come back to the H:Q later. For now, let’s move to the hamstring’s role in ACL injury prevention.
 The ACL or anterior cruciate ligament, is called such because it crosses with another ligament called the PCL or posterior cruciate ligament, making a ‘t’ shape. A 1994 study summarized the passive (non-contractile tissue) stability of the knee joint. The job of the ACL is to passively prevent 75-85% of anterior tibial shearing force on the femur above it. It also has a role in preventing tibial internal rotation and dynamic knee valgus (knocked knees).10 If you examine the picture to the right of someone’s left knee, by nature of the direction of the ACL, it will become taught if the tibia (lower bone) goes towards you or spins towards the words on the screen. Another topic of discussion is the width of the intercondylar notch and the correlation it has with ACL tears. The intercondylar notch, for our purposes, is just the upside down ‘U’ shape at the distal end of the femur in the picture. A study done in 1998 measured the width of the intercondylar notch in 714 consecutive patients who underwent ACL reconstruction using a patellar tendon graft. The 714 patients were divided into 2 groups; group 1 ≤ 15mm notch width and group 2 ≥ 16mm notch width. Twenty-three patients in group 1 and only four patients in group 2 tore their ACL in their contralateral (other) leg. An additional point of emphasis; women had statistically significant narrower notches than men.27 People with a smaller notch width have a significantly greater chance of tearing their ACLs. Athletes, clinicians, personal trainers, and coaches do not have much control of bony anatomy (scarcely do we even know the width of someone’s intercondylar notch). However, loading activities (like curtsy lunges) that can cause tibial rotation may allow the intercondylar notch to lip part of the ACL and cause injury...I don’t know, just my educated guess (COMMENT BELOW). So one prophylactic measure that everyone can take is to learn more about the movements we are doing/prescribing. Additionally, we can definitely use our hamstrings more. The two-joint hamstring muscles act to prevent anterior shear and rotation of the tibia...which is exactly the ACL’s role. If your ACL acts without the hamstring muscle’s eccentric support, than the chance of an ACL injury increases.
The ACL or anterior cruciate ligament, is called such because it crosses with another ligament called the PCL or posterior cruciate ligament, making a ‘t’ shape. A 1994 study summarized the passive (non-contractile tissue) stability of the knee joint. The job of the ACL is to passively prevent 75-85% of anterior tibial shearing force on the femur above it. It also has a role in preventing tibial internal rotation and dynamic knee valgus (knocked knees).10 If you examine the picture to the right of someone’s left knee, by nature of the direction of the ACL, it will become taught if the tibia (lower bone) goes towards you or spins towards the words on the screen. Another topic of discussion is the width of the intercondylar notch and the correlation it has with ACL tears. The intercondylar notch, for our purposes, is just the upside down ‘U’ shape at the distal end of the femur in the picture. A study done in 1998 measured the width of the intercondylar notch in 714 consecutive patients who underwent ACL reconstruction using a patellar tendon graft. The 714 patients were divided into 2 groups; group 1 ≤ 15mm notch width and group 2 ≥ 16mm notch width. Twenty-three patients in group 1 and only four patients in group 2 tore their ACL in their contralateral (other) leg. An additional point of emphasis; women had statistically significant narrower notches than men.27 People with a smaller notch width have a significantly greater chance of tearing their ACLs. Athletes, clinicians, personal trainers, and coaches do not have much control of bony anatomy (scarcely do we even know the width of someone’s intercondylar notch). However, loading activities (like curtsy lunges) that can cause tibial rotation may allow the intercondylar notch to lip part of the ACL and cause injury...I don’t know, just my educated guess (COMMENT BELOW). So one prophylactic measure that everyone can take is to learn more about the movements we are doing/prescribing. Additionally, we can definitely use our hamstrings more. The two-joint hamstring muscles act to prevent anterior shear and rotation of the tibia...which is exactly the ACL’s role. If your ACL acts without the hamstring muscle’s eccentric support, than the chance of an ACL injury increases. 
 A little more on knee valgus, as this motion is linked to ACL injury.13 There are many motions that constitute genu (knee) valgus. Hip internal rotation, hip adduction, with subsequent knee abduction are the main ones.31 As you can see in this NFL picture below, the player in the blue jersey is creating a force on the player in the white jersey, such that the tibia is being pushed forward and in, while rotating inward. These kinematics constitute both genu valgus and gruesome ACL injuries. How do you best prevent this mechanism of injury? Well one is hamstring activation, but also biomechanics. How we land, pivot, change direction, accelerate, etc. all play a part for preventing injuries. A study was conducted with 40 healthy volunteers (20 males, 20 females). The study specifically looked at landing mechanics. One group landed with a trunk flexed posture, while the other one landed in a more erect posture. They discovered that flexing the trunk during landing created an increased amount of hip and knee flexion, and this resulting flexion was significantly greater than the erect landing group at both the hip and the knee.5 Increased amounts of hip and knee flexion during landing, decreases the ground reaction force, which shields the ACL from excessive loading. More of the muscles are bearing the landing force. Our biomechanics will have an affect on the ability for our muscles to produce and absorb force. So this is a little sneak peak on how to effectively use our hamstrings, trunk flexion will have a lot to do with it. And as stated in the study above, our knee flexion angle is important in preventing ACL injuries. But having too much quadricep tension (induced by knee flexion) may be a danger within itself...this will be cleared up a little later though. For now, why knee flexion is important for ACL injury prevention. The knee flexion angle will influence the elevation angle of the ACL. The elevation angle of the ACL refers to the angle of the ACL in respect to the tibial plateau (the top part of the tibia). So pretty much as you flex your knee to 90º and beyond, the ACL is going to be essentially parallel to the tibial plateau.17,33 The change in elevation angle is super important for the ability of the ACL to accept load. The ACL will be able to sustain something called elastic deformation without injury. Elastic deformation is a special property of anything that is viscoelastic, and it refers to the temporary change in length of a structure, with a reversion back to the original shape in time. Something to note before continuing the discussion, a 1989 study displayed that the structural properties of the ACL are maximized under tensile longitudinal loading conditions and minimized under shear loading conditions.19
A little more on knee valgus, as this motion is linked to ACL injury.13 There are many motions that constitute genu (knee) valgus. Hip internal rotation, hip adduction, with subsequent knee abduction are the main ones.31 As you can see in this NFL picture below, the player in the blue jersey is creating a force on the player in the white jersey, such that the tibia is being pushed forward and in, while rotating inward. These kinematics constitute both genu valgus and gruesome ACL injuries. How do you best prevent this mechanism of injury? Well one is hamstring activation, but also biomechanics. How we land, pivot, change direction, accelerate, etc. all play a part for preventing injuries. A study was conducted with 40 healthy volunteers (20 males, 20 females). The study specifically looked at landing mechanics. One group landed with a trunk flexed posture, while the other one landed in a more erect posture. They discovered that flexing the trunk during landing created an increased amount of hip and knee flexion, and this resulting flexion was significantly greater than the erect landing group at both the hip and the knee.5 Increased amounts of hip and knee flexion during landing, decreases the ground reaction force, which shields the ACL from excessive loading. More of the muscles are bearing the landing force. Our biomechanics will have an affect on the ability for our muscles to produce and absorb force. So this is a little sneak peak on how to effectively use our hamstrings, trunk flexion will have a lot to do with it. And as stated in the study above, our knee flexion angle is important in preventing ACL injuries. But having too much quadricep tension (induced by knee flexion) may be a danger within itself...this will be cleared up a little later though. For now, why knee flexion is important for ACL injury prevention. The knee flexion angle will influence the elevation angle of the ACL. The elevation angle of the ACL refers to the angle of the ACL in respect to the tibial plateau (the top part of the tibia). So pretty much as you flex your knee to 90º and beyond, the ACL is going to be essentially parallel to the tibial plateau.17,33 The change in elevation angle is super important for the ability of the ACL to accept load. The ACL will be able to sustain something called elastic deformation without injury. Elastic deformation is a special property of anything that is viscoelastic, and it refers to the temporary change in length of a structure, with a reversion back to the original shape in time. Something to note before continuing the discussion, a 1989 study displayed that the structural properties of the ACL are maximized under tensile longitudinal loading conditions and minimized under shear loading conditions.19  If we take a gander to our right, we will see the patellar tendon (representing quadricep pull for our understanding), ACL, and biceps femoris pull, all in order from left to right in the picture. Let’s not get lost in the trigonometry, just know this...as the knee progresses into extension (figure ‘a’), the ACL elevation angle is increased (the middle arrow). As you can see by the force vector arrow on the left of figure ‘a’, by nature of the configuration, the anterior force generated by the patellar tendon on the tibia, resisted by the ACL, is more of a shear force as the tibia is being pulled anteriorly. As we determined above, shear loading minimizes the structural properties of the ACL (it can’t work as well). On the flip side, if we go to figure ‘b’, we will see forces that reside with knee flexion. With knee flexion, the ACL elevation angle decreases, along with the shear component of the resultant ACL force, while the tensile component increases. In figure ‘b’, the patellar tendon force is no longer anterior, yet a little posterior. Further aiding the case for knee flexion, the force vector on the right in figure ‘b’ represents the now almost absolute posterior pull generated by the biceps femoris. This posterior pull will aid the ACL in preventing the tibia from rotating inward and shearing anteriorly.33 To summarize, greater degrees of trunk flexion while landing increases your hip and knee flexion, while decreasing genu valgus. This leads to a decrease in ground reaction force, due to force absorption by your muscles in the lower extremity. The knee flexion in itself also decreases the patellar tendon anterior shear force, decreases the ACL elevation angle (allowing it to act more longitudinal, therefore maximizing its structural capabilities), and increasing the posterior force vector elicited by the bicep femoris, all acting to shield your ACL from injury...how nice is that. Now, something that you may or may not have noticed is the anterior force vector of the patellar tendon (the quadriceps) early in flexion (figure ‘a’). I am going to hypothesize, for multiple reasons, that we want to minimize the quadriceps activation early on in flexion...let’s dive a little deeper. A 1999 study demonstrated in the cadaveric (human cadaver) knee, during coactivation of the hamstrings and quadriceps, the amount of tibia anterior translation and ACL stress was significantly less when compared to an isolated quadriceps contraction from 15–60° of knee motion.18 Too much quadriceps pull, too early in the range of knee flexion, without the counter activity of the hamstrings, may be a risk factor for ACL injury. This matches with the study and picture from above. Further attenuating this, a 2006 study displayed that a simulated eccentric hamstring contraction in cadavers reduced the strain on the ACL.30 Even further, a 1992 study determined that ACL strains increased with quadriceps contraction and was less if the quadriceps and hamstrings contracted simultaneously.3 Also multiple studies have demonstrated that ACL injuries and hamstring strains can be caused by the hamstrings not generating equal force eccentrically, countering the concentric torque that the quadriceps apply to the tibia.1,7,24,25 I think it is important to revisit a statement that I made in the beginning of the story, as I was discussing the hamstring anatomy, “The long head of the biceps femoris, semitendinosus, and semimembranosus are called two-joint muscles. As we reviewed, these muscles will in turn act on both the hip and the knee. Another important implication of two-joint muscles is that they can be shortened and lengthened differently at each joint. For example, when you squat, you are simultaneously flexing your knee and hip on the way down. Therefore, you are simultaneously shortening the long head of the biceps femoris, semitendinosus, and semimembranosus distally at the knee, and lengthening them at the hip.” So, how do we apply this? We want to increase hamstring force absorption during landing but still need to bend our knees to optimize the three force vectors from the image above. If you have more hip flexion than knee flexion, there may be a net eccentric force and an increase in passive tension by the hamstrings (COMMENT BELOW). Those were some examples in which too much quadriceps tension/activation, too early within the range of knee flexion, can be harmful for at least ACL injuries. However, my hypothesis is only partially proven. We can increase comprehension by looking at another mechanism of injury.
If we take a gander to our right, we will see the patellar tendon (representing quadricep pull for our understanding), ACL, and biceps femoris pull, all in order from left to right in the picture. Let’s not get lost in the trigonometry, just know this...as the knee progresses into extension (figure ‘a’), the ACL elevation angle is increased (the middle arrow). As you can see by the force vector arrow on the left of figure ‘a’, by nature of the configuration, the anterior force generated by the patellar tendon on the tibia, resisted by the ACL, is more of a shear force as the tibia is being pulled anteriorly. As we determined above, shear loading minimizes the structural properties of the ACL (it can’t work as well). On the flip side, if we go to figure ‘b’, we will see forces that reside with knee flexion. With knee flexion, the ACL elevation angle decreases, along with the shear component of the resultant ACL force, while the tensile component increases. In figure ‘b’, the patellar tendon force is no longer anterior, yet a little posterior. Further aiding the case for knee flexion, the force vector on the right in figure ‘b’ represents the now almost absolute posterior pull generated by the biceps femoris. This posterior pull will aid the ACL in preventing the tibia from rotating inward and shearing anteriorly.33 To summarize, greater degrees of trunk flexion while landing increases your hip and knee flexion, while decreasing genu valgus. This leads to a decrease in ground reaction force, due to force absorption by your muscles in the lower extremity. The knee flexion in itself also decreases the patellar tendon anterior shear force, decreases the ACL elevation angle (allowing it to act more longitudinal, therefore maximizing its structural capabilities), and increasing the posterior force vector elicited by the bicep femoris, all acting to shield your ACL from injury...how nice is that. Now, something that you may or may not have noticed is the anterior force vector of the patellar tendon (the quadriceps) early in flexion (figure ‘a’). I am going to hypothesize, for multiple reasons, that we want to minimize the quadriceps activation early on in flexion...let’s dive a little deeper. A 1999 study demonstrated in the cadaveric (human cadaver) knee, during coactivation of the hamstrings and quadriceps, the amount of tibia anterior translation and ACL stress was significantly less when compared to an isolated quadriceps contraction from 15–60° of knee motion.18 Too much quadriceps pull, too early in the range of knee flexion, without the counter activity of the hamstrings, may be a risk factor for ACL injury. This matches with the study and picture from above. Further attenuating this, a 2006 study displayed that a simulated eccentric hamstring contraction in cadavers reduced the strain on the ACL.30 Even further, a 1992 study determined that ACL strains increased with quadriceps contraction and was less if the quadriceps and hamstrings contracted simultaneously.3 Also multiple studies have demonstrated that ACL injuries and hamstring strains can be caused by the hamstrings not generating equal force eccentrically, countering the concentric torque that the quadriceps apply to the tibia.1,7,24,25 I think it is important to revisit a statement that I made in the beginning of the story, as I was discussing the hamstring anatomy, “The long head of the biceps femoris, semitendinosus, and semimembranosus are called two-joint muscles. As we reviewed, these muscles will in turn act on both the hip and the knee. Another important implication of two-joint muscles is that they can be shortened and lengthened differently at each joint. For example, when you squat, you are simultaneously flexing your knee and hip on the way down. Therefore, you are simultaneously shortening the long head of the biceps femoris, semitendinosus, and semimembranosus distally at the knee, and lengthening them at the hip.” So, how do we apply this? We want to increase hamstring force absorption during landing but still need to bend our knees to optimize the three force vectors from the image above. If you have more hip flexion than knee flexion, there may be a net eccentric force and an increase in passive tension by the hamstrings (COMMENT BELOW). Those were some examples in which too much quadriceps tension/activation, too early within the range of knee flexion, can be harmful for at least ACL injuries. However, my hypothesis is only partially proven. We can increase comprehension by looking at another mechanism of injury.
The injury mechanism I am speaking of is called chondromalacia patella (also known as patellofemoral pain syndrome, or PFPS). The patella’s purpose is to increase the moment arm of the quadriceps tendon, leading to an increased torque potential by the quadriceps for knee extension. There are a few theories surrounding patellofemoral pain. One is damage to the pre-patellar surface or periosteum on the femur. Both of these can be tackled similarly, with a biomechanical approach. Stepping away from biomechanics for a moment, it would be inappropriate to ignore that this disorder may be largely psychosomatic in nature. There is a plethora of research, that I am not going to go into now (will in the future), but it discusses the psychoneurological phenomenon that may be PFPS. This model has been shown extensively with other physical pain manifestations in the body, including low back pain. Despite this, there are many correlations that PFPS has with biomechanical variables. In my opinion, it’s probably a slippery mix of both. For now, we will talk about what is going on biomechanically in the musculoskeletal system.
In the beginning of knee flexion from full extension, the patella (knee cap) is in contact with the periosteum of the femur (the connective tissue that surrounds the outer portion of the thigh bone). This is the time where clinicians usually say that the pre-patellar surface is susceptible to damage from increased force of the quadriceps causing or exacerbating PFPS. But in actuality, when you look at the force vector of the patellofemoral joint reaction force (PFJRF - the force that the patella exudes on the femur) due to pull of the quadriceps in this position, it is quite minimal just by nature of the patella in relation to the femur, and the direction of pull by the quadriceps. This concept is interesting, and should be talked about when discussing explanations for pain in exercises that involve TKE (terminal knee extension). In this story, we will find a few biomechanical sources of PFPS and eventually tie it back to the hamstrings. These include examples of lateral patellar tracking as a means of increasing PFJRF and examples not including a frontal plane (side to side if you are looking straight at the knee) component causing increased PFJRF. We will talk about both separately, but the goal of each is the same...decreased PFJRF leads to a decreased PFPS symptoms.
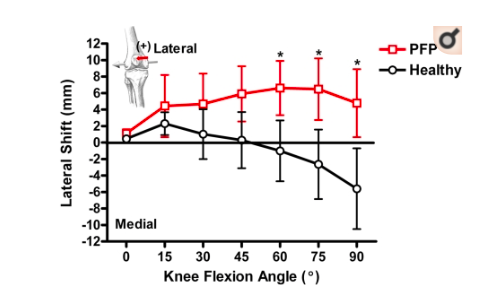
Extremely brief background; as you flex the knee, the patella goes inferiorly (down), as you extend the knee, the patella goes superiorly (up). As the patella tracks the femur, the patella and femur continuously amend their surface area overlap. This will have implications for PFJRF; think about stepping on a single nail v.s. a bed of nails. Let’s start with lateral subluxation of the patella. As knee flexion increases from 30-90 degrees, there is stability in both the medial and lateral facets of the femoral trochlea. Where problems can arise is when the patella subluxes over the lateral facet causing anterior knee pain. One reason that this can happen is an increased Q-angle, which is the angle created by the line of the tibial tubercle (bony prominence in in which the patellar tendon attaches on the tibia) to the middle of the patella and the line from the middle of the patella to the ASIS (anterior superior iliac spine) on the pelvis. If the Q-angle is too high than this may cause a pull of the patella off of it’s normal track, causing the patella glide over the lateral distal femur leading to pain during knee motion. Let’s examine a study looking at in vivo and noninvasive patellar tracking patterns in both participants with and without symptoms of patellofemoral pain. Participants with symptoms of patellofemoral pain, at 90 degrees of knee flexion, had patellas that had significantly more lateral translation (5.05±3.73mm), as compared to the non-pain healthy controls (-4.93±3.93mm).29 This study offered a graph as seen above; it really pronounces the correlation that is drawn between patellofemoral pain and lateral patellar tracking. Why is this lateral tracking of the patella during knee flexion painful? The back of the patella can be shearing against the lateral facet of the femoral trochlea (the bony prominence that the patella runs over during knee flexion activities). Many things can cause this to happen and be painful, however I will not be going extensively into the literature of each: shallow lateral trochlea, increased Q-Angle (net direction of pull exhibited by the quadriceps), an imbalance of the vastus lateralis and medialis (2 of the quadricep muscles). Additionally, a tight iliotibial band can cause lateral patellar deviation due to its attachment to the lateral aspect of the patella.16 I am sure there are multiple courses of action to help this problem. You can probably make a case for adding more bone to your lateral trochlea (half kidding), using russian stim on the vastus lateralis, foam rolling your tensor fascia latae, etc. (COMMENT BELOW). One idea that we can implement is decreasing the amount of pull that the quadriceps tendon is having on the patella. This may decrease the lateral tracking of the patella and decrease the PFJRF. Decreasing quad tension may also decrease symptoms even if the patella is not tracking laterally. More on this after a deeper analysis of lateral patellar tracking.
 Look at the image to the left for context in the following discussion. If QS (lateral shear force due to the quadriceps pull) and TS (lateral shear force due to the patellar ligament) are both greater than 0, then that deduces a greater RL force than RM force, which will cause a net lateral force. The higher the Q-Angle, the higher the RL/RM ratio. If the resultant force is lateral, this can cause lateral patellar tracking and chondromalacia. Further, the resultant forces on the patella due to the quadriceps and the patellar ligament are not linear; this is a laterally directed force on the patella (image below on the right). If there is a great amount of valgus angle in the frontal plane, the Q-Angle will increase. This increase in lateral force increases the ability of the patella to sublux laterally. Some good things happen though when the knee is flexed. Once knee flexion reaches about 90º, the contact area between the patella and the femur increases, as the patella shifts cranially.11,15 This is going to compensate for the increased PFJRF as the knee is flexed to 90º (standing on a bed of nails, rather than one nail). We still have to be cautious of too high of a quadricep force at 90º. Normal kinetics include a diminishment in quadriceps tension after 90º of flexion because the patella should start to sink into the intercondylar notch, therefore decreasing the moment arm of the quadriceps tendon.11,12 Does this mean that too high of a quadriceps force inhibits the patella from entering the notch, leading to an increase in quadriceps tension and PFJRF, with knee flexion that follows? It is important to understand that increased quad tension will increase PFJRF, and this is all independent of lateral patellar tracking. So let’s think.
Look at the image to the left for context in the following discussion. If QS (lateral shear force due to the quadriceps pull) and TS (lateral shear force due to the patellar ligament) are both greater than 0, then that deduces a greater RL force than RM force, which will cause a net lateral force. The higher the Q-Angle, the higher the RL/RM ratio. If the resultant force is lateral, this can cause lateral patellar tracking and chondromalacia. Further, the resultant forces on the patella due to the quadriceps and the patellar ligament are not linear; this is a laterally directed force on the patella (image below on the right). If there is a great amount of valgus angle in the frontal plane, the Q-Angle will increase. This increase in lateral force increases the ability of the patella to sublux laterally. Some good things happen though when the knee is flexed. Once knee flexion reaches about 90º, the contact area between the patella and the femur increases, as the patella shifts cranially.11,15 This is going to compensate for the increased PFJRF as the knee is flexed to 90º (standing on a bed of nails, rather than one nail). We still have to be cautious of too high of a quadricep force at 90º. Normal kinetics include a diminishment in quadriceps tension after 90º of flexion because the patella should start to sink into the intercondylar notch, therefore decreasing the moment arm of the quadriceps tendon.11,12 Does this mean that too high of a quadriceps force inhibits the patella from entering the notch, leading to an increase in quadriceps tension and PFJRF, with knee flexion that follows? It is important to understand that increased quad tension will increase PFJRF, and this is all independent of lateral patellar tracking. So let’s think. 

I am going to speculate, as I do not have definitive research for the following thought process. First, a study looking at the contributions of the sagital (front to back) plane patellar motion in participants with and without PFPS; they had some interesting findings. It was described in the study that the patella moves similarly in both groups from 0-90º of knee flexion, yet the kinematics change past that. The healthy controls exhibited a significantly greater amount of patellar sagittal plane motion from 90-120º; the mean patellar motion angle was 23.6° in the volunteer group and 18.5° in PFPS group.21 My question: normally after 90º of knee flexion, the patella starts to sink into the intercondylar notch, and this ultimately begins to decrease the tension of the quad with subsequent degrees of knee flexion. If people with PFPS can decrease the amount of net superior translation that the quadriceps elicit on the patella, would this allow for normal patellar movement into the notch, decreasing quadricep tension, PFJRF, and pain? Not sure, but it is about the hamstrings right now, so I like the thought process (COMMENT BELOW).
In conclusion, excessive quadriceps pulling force, too early in knee flexion, will have kinematic and kinetic implications. It will lead to increased anterior translation of the tibia, and put stress on the ACL before 90º of knee flexion. At this point the ACL is not in its optimal structural configuration. Additionally, it will lead to significantly more lateral displacement of the patella at 90º of knee flexion, increasing PFJRF and pain. Finally, it will result in decreased patellar inferior glide at 90º, further increasing quadriceps pulling force, PFJRF and pain. The evidence/biomechanics speak to my hypothesis from before.
If we review the anatomy, the hamstrings are 4 muscles that attach to this bony prominence on the pelvis called the ischial tuberosity. This attachment of your 4 hamstrings (semimembranosus, semitendinosus, long head of the biceps femoris, ischial portion of the adductor magnus) act as a powerful group of hip extensors. Activating your hamstrings, along with the rest of the posterior chain, can allow for some great eccentric control. Great enough that you can control the eccentric portion of movement (like lowering yourself into a squat) with the hip extensor muscles (hamstrings and glutes) rather than over relying on the knee extensors (quadriceps). Two great things are happening if we can manage this. One is that we are getting the great muscle work in the hamstring group for all of the injury prevention and performance optimization that we talked about earlier. Two, when it comes to PFPS and ACL injury prevention, we want to decrease the tension of the quadriceps tendon in knee flexion from 0-90º. Doing so may decrease the PFJRF, decrease the amount of lateral tracking that the patella has, decrease anterior tibial shear, therefore decreasing the unwanted stress that is associated with PFPS and ACL injuries.
The way I would approach this biomechanically is different depending on the task. We already went into the appropriate ways to land in order to minimize ACL stress. If we want to do a move like a lunge or a squat, I would start the movement with minimal knee flexion (don’t get any ankle dorsiflexion). And have enough hip flexion that you are keeping the center of gravity (COG) over the mid foot. So from the side your tibia should be straight up and down, and your hips will be flexed according to the COG. By doing this, you are shifting the load from your quadriceps to your hip extensors as much as you can. Once you reach 90º of knee flexion, the quad tendon force will begin to decrease because the patella is sinking into the intercondylar notch. This is the best time to start to increase depth by bringing your knees forward (increasing dorsiflexion), and obtaining a more upright torso (whatever hip position that keeps the weight over the mid foot). On the way back up, if you recreate your horizontal torso angle as the first move by leaning forward (eccentric activation of hamstrings) and then begin hip extension, this will minimize PFJRF on the way up. The knee just goes for a ride, while the hips do the lifting. If the weight that a client of mine was using inhibited this motor pattern at the knee or at least some resemblance of it, I would certainly decrease the weight...that’s how important it is. If someone that I train develops PFPS from lifting, when the purpose of lifting is to work on your body, movement, and overall health, then that would be counterintuitive. CHECK OUT MY YOUTUBE VIDEO ON SQUATTING.
Staying on that note, only knowing one piece to the puzzle can be perilous. This story was mainly about the hamstrings and the knee joint, but you need to consider the hips and lumbar spine as well. If you do not have proper hip flexion ROM and you attempt to squat in this nature, you will compensate at the lumbar spine early in the movement. This brings upon two issues. One, this is the reason people are scared of big moves like the squat and deadlift, but if you do them appropriately with an awesome trainer/therapist, you will reap the benefits. Two, some therapists and trainers are very black and white in my experience. Many live and die with studies that come out on JOSPT (Journal of Orthopedic and Sports Physical Therapy) without any context on how they conducted the study, nor any attempt to gain their own understanding. For example, saying posture doesn’t matter because that was a headline in a JOSPT study. I can give you 100 instances where posture (dynamic or static; foot or head; mental or physical; etc.) matters, and 100 where you can ignore it, instead of making definitive conclusions based on a headline. Further, the “imaging doesn’t matter” movement, is pure discrimination. Image of what? Taken by what? Showing what? Those questions are scarce. We need to strive more in order to gain context. So when it comes to bringing your knees forward or not during a squat, don’t relay someone else's conclusion. Look at the research AND the unbiased physics AND your own experience, rather than playing a big game of telephone (a game where words get twisted as they travel from one ear to the next). No one is perfect, but by doing your due diligence you are doing the very best you can to keep your athletes/clients/patients at a high level and safe...DON’T BE A ROBOT.
Moving on from my rant, ask anyone who has had pain from a hamstring strain or PFPS, not fun. ACL injuries are even worse. We know that having hamstring strength in ranges of knee motion are vital to both preventing these injuries and increasing performance...so, how do we do this? If you lift, land, and move correctly, while constantly trying to improve your range of motion during those movements, you will develop great strength in ranges of motion for many muscles and joints. You may be all researched out, but one more to prove this notion. In a 2010 randomized controlled trial looking at the difference between active stretching v.s. passive stretching for the hamstring muscles, they found significant differences in range of motion (ROM) gains and maintenance of those gains. The subjects included in the study had tight hamstring muscles. This was categorized as having a knee extension angle of less the 160º while in 90º of hip flexion. The experimental group (active stretching) consisted of sitting in the position of 90º hip flexion and actively extending their knee with the quadriceps muscles. This group completed 4 repetitions, with 30 second isometric holds on each leg, twice a day, for 4 days/week. The control group (passive stretching) consisted of two exercise, with the same frequency of exercise prescription as the experimental group but they had a total of 12 repetitions/day while the experimental group only had a total of 8. Despite this, the active stretching group showed significantly better increases in hamstring ROM and maintained those increases almost completely, 4 weeks after the active stretching program. The control group however, nearly lost all of the little range of motion that they had gained at 4 weeks following the intervention.20 Explanations include: antagonist contraction will further relax the muscle being stretched, having antagonist strength within a greater ROM will help to maintain ROM, and doing so in a position that demands greater body control, allows for ROM changes.
If I needed to lengthen someone’s hamstrings, I would do it with the same exercise almost every time...the Romanian Deadlift. Your using the bend movement pattern and eccentrically controlling the descent of the weight with your hamstrings and probably some isometric of your quadriceps. The reason why this is a great way to gain range, or better said strength in range, is because you are using, not only stretching techniques, but also you are using movement coordination, strength, balance, and proprioception while you are trying to acquire greater ranges of motion. CHECK OUT MY YOUTUBE VIDEO ON ROMANIAN DEADLIFTS.
In essence, research is just a combination of trends and correlations that people search for. Biomechanical and experiential explanations definitely aid in our understanding of these trends. Yet, nothing is clear cut, and many variables are more difficult to control. You can sustain hamstring strains, PFPS, and ACL injuries by having or lacking strong hamstrings within the range of knee motion. If a great enough force is applied, I don’t care how strong your hamstrings are, they will still tear. We also talked about the increased susceptibility one has to ACL injury if their intercondylar notch is narrow. Finally, we discussed PFPS and the psychosomatic disorder that it might be. All you can do in this whole thing is the best you can. Strengthening the hamstrings within ranges might not prevent injury, but it might. And I’ll bet money that it won’t hurt.
I had a blast creating this story/review to connect the research and biomechanics for this discussion. There are a plethora of well thought out points. However, this is absolutely NOT the end-all-be-all for this discussion, nor some of the mini discussions within it. If you are a healthcare professional, or anyone for that matter, please give feedback and criticism (I can take it) to the story of the hamstrings, as this will offer the greatest amount of value to anyone that reads it. All I ask is to include supported research, your own clinical/professional experience, and/or biomechanical mechanisms of action.
Sincerely,
ROSSY G.
References
- Aagaard, P. et al. A new concept for isokinetic hamstring: Quadriceps muscle strength ratio. Am J Sports Med.1998. 26: 231–237.
- Aagaard, P., Simonsen E.B., Trolle, M., Bangsbo, J., Klausen, K. Isokinetic hamstring/quadriceps strength ratio: Influence from joint angular velocity, gravity correction and contraction mode. Acta Physiol Scand.1995. 154: 421–427.
- Beynnon, B. et al. The measurements of anterior cruciate ligament strain in vivo. Int Orthop.1992. 16, 1-12.
- Beynnon, B.D., Fleming, B.C., Johnson, R.J., Nichols, C.E., Renstrom, P.A., Pope, M.H. Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am. J. Sports Med.1995. 23, 24– 34.
- Blackburn, J. Troy, Padua, Darin A. Influence of trunk flexion on hip and knee joint kinematics during a controlled drop landing. Clinical Biomechanics.2007. 313-319.
- Brockett, C. L., D. L. Morgan, and U. Proske. Predicting Hamstring Strain Injury in Elite Athletes. Med. Sci. Sports Exerc.2004. Vol. 36, No. 3, pp. 379–387.
- Coombs, R. and Garbutt, G. Development in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J Sports Sci and Med.2002. 1:56–62.
- Croisier, J.L., Forthomme, B., Namurois M.H., Vanderthommen M., Crielaard J.M. Hamstring muscle strain recurrence and strength performance disorders. Am J Sports Med 30.2002. 199–203.
- Croisier J.L., Ganteaume, S., Binet, J., Genty, M., Ferret, J.M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am J Sports Med 36.2008. 1469–1475.
- Fu et al. Biomechanics of the knee ligaments: Basic concepts and clinical application. Instr Course Lecture.1994. 43, 137-148.
- Goodfellow, J. et al. Patellofemoral joint mechanics and pathology. 1. Functional anatomy of the patellofemoral joint. J Bone Joint Surg.1976. 58, 287.
- Hehne, H.J. Biomechanics of the patellofemoral joint and its clinical relevance. Clin Orthop.1990. 258, 73-85
- Hewett, T.E., Myer, G.D., Ford, K.R., Heidt, R.S., Colosimo, A.J., McLean, S.G., van den Bogert, A.J., Paterno, M.V., Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes. Am. J. Sports Med.2005. 33, 492–501.
- Kean, C., Fox, J., Borges, N., Stanton, R., and Scanlan, A. Decrements in hamstrings strength are associated with decreased performance during simulated basketball game-play. Journal of Science and Medicine in Sport.2017. 20, e50.
- Komistek, R.D. et al. An in vivo determination of patellofemoral contact positions. Clin Biomech.2000. 12, 118-124.
- Kwak, S.D. et al. Hamstrings and iliotibial forces affect knee ligaments and contact pattern. J Orthop Res.2000. 18, 101-118.
- Li, G., Papannagari, R., DeFrate, L.E., Yoo, J.D., Park, S.E., Gill, T.J. Comparison of the ACL and ACL graft forces before and after ACL reconstruction: an in vitro robotic investigation. Acta Orthop.2006. 77, 267–274.
- Li, G., Rudy, M.S., Kanamori, A., B, M.C., Woo, S.L.-Y. The importance of quadriceps and hamstring muscle loading on knee kinematics and in situ forces in the ACL. J. Biomech.1999. 32, 395– 400.
- Lyon, R.M., Woo, S.L., Hollis, J.M., Marcin, J.P., Lee, E.B. A new device to measure the structural properties of the femur-anterior cruciate ligament-tibia complex. J. Biomech. Eng.1989. 111, 350–354.
- Meroni, R. et al. Comparison of Active Stretching Technique and Static Stretching Technique on Hamstring Flexibility. Clin J Sport Med.2010. Volume 20, Number 1.
- Narkbunnam, R. et al. Sagittal plane evaluation of patellofemoral movement in patellofemoral pain patients with no evidence of maltracking. Knee Surgery Sports Traumatol.2013.
- Neuman, D. Journal of Orthopaedic & Sports Physical Therapy.2010. Volume:40 Issue:2 Pages:82–94
- Nordin, M. and Frankel, V. Biomechanics of the Musculoskeletal System 4th Edition.
- Ruas, C.V., Minozzo, F., Pinto, M.D., Brown, L.E., Pinto, R.S. Lower-extremity strength ratios of professional soccer players according to field position. J Strength Cond Res.2015. 29: 1220–1226.
- Ruas, C.V., Pinto, M.D., Brown, L.E., Minozzo, F., Mil-Homens, P., Pinto, R.S. The association between conventional and dynamic control knee strength ratios in elite soccer players. Isokinet Exerc Sci.2015. 23(1):1–12.
- Seward, H., J. Orchard, H. Hazard, and D. Collinson. Football injuries in Australia at the elite level. Med. J. Aust.1993. 159:298–301.
- Shelbourne, D. The Relationship Between Intercondylar Notch Width of the Femur and the Incidence of Anterior Cruciate Ligament Tears. American Journal of Sports Medicine.1998. Vol, 26. No. 3.
- Taylor, Jeffrey et al. Prevention of Lower Extremity Injuries in Basketball: A Systematic Review and Meta-Analysis. Sports Health.2015.
- Wilson, Nicole et al. In Vivo Noninvasive Evaluation of Abnormal Patellar Tracking During Squatting in Patients with Patellofemoral Pain. J Bone Joint Surg Am.2009. 91(3): 558–566.
- Withrow, T.J., Huston, L.J., Wojtys, E.M., Ashton-Miller, J.A. A lengthening hamstring contraction condition reduces ACL strain in an in vitro jump landing model: an ACL protective mechanism, J. Orthop. Res. Trans.2006. 31, Paper No. 1124. 52nd Annual Meeting of the Orthopaedic Research Society, Chicago, IL.
- Zeller, B.L., McCrory, J.L., Kibler, W.B., Uhl, T.L. Differences in kinematics and electromyographic activity between men and women during the single-legged squat. Am. J. Sports Med.2003. 31, 449–456.
- Zernicke, R.F. et al. Human patellar tendon rupture. J Bone Joint Surg Am.1977. 59, 179-183.
- Zheng, N., Fleisig, G.S., Escamilla, R.F., Barrentine, S.W. An analytical model of the knee for estimation of internal forces during exercise. J. Biomech.1998. 31, 963–967.
Comments
Post a Comment